TGA recommends loosening rules on psychedelic-assisted therapy - fewer psychiatry hours, broader workforce, what it means for EMD
The TGA (Australia's drug regulator) just recommended a set of big changes for MDMA and psilocybin-assisted therapies in Australia…
The exact same space our Investment Emyria (ASX: EMD) is rolling out clinics in.
(source)
The three biggest recommendations:
1. The on-site therapy team of 2 - including one registered therapist is broader.
Today, two therapists oversee each session - typically a psychologist and a counsellor.
The TGA wants to widen the eligible pool.
Clinical psychologists, GPs, mental health nurses or occupational therapists could form part of the team under these proposed changes.
The prescribing psychiatrist can also add psychotherapists, counsellors, social workers and other health health workers.
2. The prescribing psychiatrist doesn't have to stay on-site for the whole session.
Right now the prescribing psych has to remain at the clinic the entire time.
The TGA is recommending the psych can leave once the drug is ingested.
Under the proviso that the patient stays within 15 minutes of an emergency room.
3. The pathway to becoming an AP is more clearly defined.
Psychiatrists would be able to qualify via clinical-trial involvement OR through supervised psychedelic-assisted psychotherapy with an experienced authorised prescriber.
Why this matters specifically for EMD
First of all, these are recommendations, not yet rules, and they will need further approvals before they are put into action.
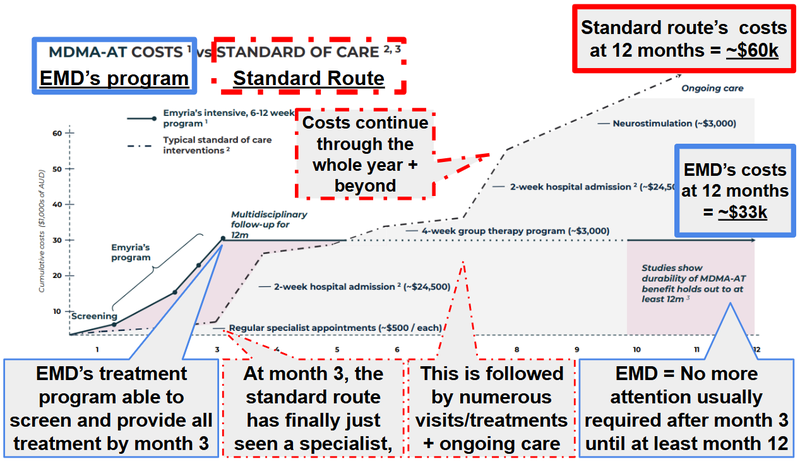
The reason we think it could be a big positive change for EMD is because the biggest commercial headwind on psychedelic-assisted therapy in Australia is cost.
The industry estimates put a full course of treatment at around A$30,000.
EMD itself’s treatment is around that mark and they themselves have indicated that conventional treatment options (non psychedelic-assisted therapy), can be double this over 12 months:
(source)
That price tag is driven mostly by:
- Workforce intensity.
- Hours of psychiatrist time.
- Hours of paired-therapist time.
- All under strict on-site supervision.
- Across multiple dosing sessions per treatment course.
Cost determines two things that matter most for EMD's path to scale:
How many patients can practically access the treatment and how cheaply EMD can deliver it inside its private health insurer (Medibank) and government payer (Department of Veterans' Affairs) reimbursement envelopes.
So:
- Less psychiatry-time per session = better unit economics.
- More eligible mental health professionals = a deeper hiring pool for clinic workforce.
- Off-site supervision (under tight conditions) = one psychiatrist could potentially cover more throughput per day.
In the article, clinical psychologist Monica Schweickle (director of Peridot Clinic) was quoted on exactly this:
(source)
EMD is in a strong position to benefit if the recommended changes get adopted
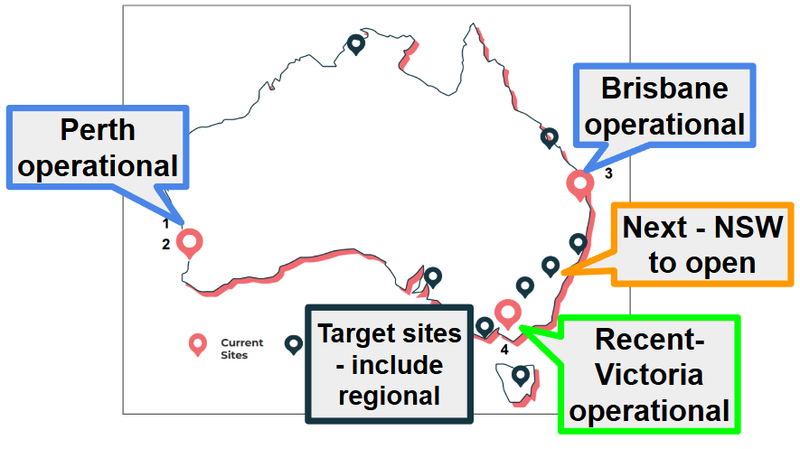
EMD’s currently got clinics across Brisbane, Perth and Victoria PLUS has clinics planned for NSW.
(source)
And right now EMD has a lead in the industry because:
- TGA authorisation to deliver MDMA-assisted care to patients (hard to get).
- Payer agreements with Medibank and DVA (Department of Veteran Affairs is the world's first government-payer reimbursement for psychedelic treatments).
- Data that shows it works - ~67% durable remission at 12+ months and ~76% clinically significant benefit from EMD's published PTSD outcomes.
- A means to deliver therapies through clinics EMD owns or operates (Perth, Brisbane, Mornington via Avive Health, NSW signed with Matilda Nepean).
- Scale potential with an approved protocol EMD can "franchise" to other clinics looking to deliver psychedelic-assisted therapy.
A wider eligible workforce makes point #4 easier. It also makes point #5 more valuable.
The macro picture is moving in the right direction too for EMD
This is the second material policy tailwind for EMD in roughly five weeks.
On 18 April, President Trump signed an Executive Order to accelerate research and access to psychedelic medicine in the US.
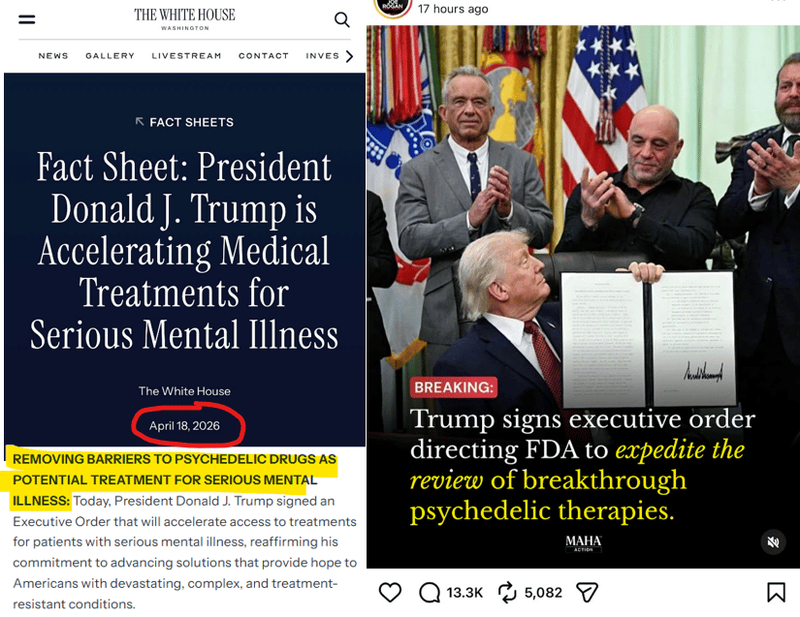
See our most recent EMD article, which we did immediately following this news: EMD: USA signs exec order to fast-track psychedelic medicine research and access. EMD is already doing it.
This development made EMD's global partnership program suddenly more strategically valuable.
Overseas drug developers can use EMD's clinic networks to run trials, because EMD already has the proven capabilities (and is legally allowed to here).
What’s next for EMD?
Here is everything we are looking out for over the next few months from EMD:
- VIC clinic treatments commence - (Now Operating).
- NSW clinic treatments commence (post the current therapist recruitment drive, 7 psychiatrists confirmed for NSW training ahead of commencing).
- More payers - EMD is already working with Workcover Australia (including the Australian Federal Police's cohort, one of the highest PTSD-burden groups in the country). A third major payer after Medibank + the Department Of Veterans’ Affairs could also be a meaningful re-rate catalyst
- The BIG new one after the recent US news: Any US-facing deal. Given the Trump EO, this is the catalyst we were previously only hoping for - now we think it's a "when" more than an "if."